Axial Arthritis
<-Appendicular Arthritis | Lucent Lesions of Bone->
In the appendicular skeleton, one is mostly concerned with the diarthrodial synovial joints. While this type of joint is also found in the axial skeleton (the facet (a.k.a. aphophyseal) joints and portions of the sacroiliac joints), there are also many amphiarthrodial joints which are not synovial (the intervertebral disc joints). However, there are several structures in the intervertebral disc joint which are analogous to structures found in a true synovial joint. The cartilaginous endplate, the annulus fibrosus, and the nucleus pulposus are analogous to the articular cartilage, the joint capsule and the synovial fluid of the synovial joint.
The different anatomy and physiology of these joints means that we will see different disorders affecting this part of the skeleton. However, the same basic logical principles mentioned in the last chapter also apply here.
Degenerative disorders
Osteoarthritis
This is, by far, the most common type of arthritis seen in humans. By definition, osteoarthritis occurs in a synovial joint. In the spine, therefore, osteoarthritis occurs in the apophyseal (facet) joints, the uncovertebral joints (cervical spine), the costovertebral joints, and the sacroiliac joints. Osteoarthritis may be primary or secondary.

marked osteophytosis and joint space narrowing is noted in the facet joints in this patient with severe osteoarthritis of the lumbar spine — the osteophytosis is causing significant encroachment on the lateral recesses bilaterally
Degenerative nuclear disease
Another very common disorder is degeneration of the nucleus pulposus. With age, the nucleus tends to become more and more dehydrated, and gradually begins to degenerate. As this happens, the intervertebral disc height begins to decrease. When this happens, the altered pattern of stresses may lead to marginal osteophytosis adjacent to the affected endplates. As the disc space decreases in height, increased stress is also placed on the facet joints, leading to the frequent association of osteoarthritis of the facets at the same level.
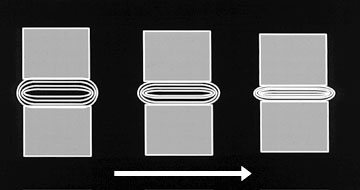
with increasing age (arrow), progressive degeneration of the nucleus leads to decreasing disk space height
Degenerative annular disease
Yet another extremely common degenerative disorder involves degeneration of the annulus fibrosus. This leads to marginal osteophytosis at the endplates, especially in the thoracolumbar spine in many persons over 50 years of age. In the literature, this entity has been termed “spondylosis deformans” or “senile ankylosis”. However, both of these terms tend to make the disease sound a lot worse than it really is. Using these terms in a film report can lead to calls from clinicians wondering just what horrible disease their patients have. Therefore, I prefer to state “marginal osteophytes are noted at multiple disc spaces in the spine” in my dictations. The clinicians know what I’m describing and they and their patients are not unduly frightened by the unfamiliar terminology used for this very familiar process.
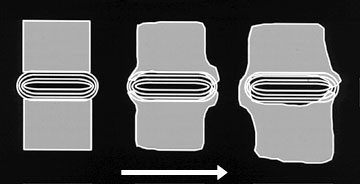
with increasing age (arrow), progressive degeneration of the annulus leads to increasing osteophytosis at the disk space margins — the height of the disk space is largely preserved
In practice, one often sees evidence of degeneration of both the annulus and the nucleus. It usually doesn’t make a lot of difference to the referring clinician which component of the disk has degenerated. Therefore, I suggest using the term “degenerative disk disease” in one’s dictations to refer to these entities.

marked marginal osteophytosis is noted at each disk space in this patient with predominantly annular degeneration

disk space narrowing is noted at multiple levels in this patient with degenerative disk disease — a thin linear area of lucency in the L4-5 disk space represents gas in the degenerated disk
Diffuse Idiopathic Skeletal Hyperostosis (DISH)
DISH is an extremely common entity of unknown etiology, which manifests itself by ossification of the anterior longitudinal ligament, which produces large flowing bony excrescences along the spine, especially the anterior aspect.
Inflammatory spondyloarthropathies
Rheumatoid arthritis
This is a disorder of unknown etiology characterized by synovial inflammation, pannus formation, and then destruction of bone and cartilage.
Ankylosing spondylitis
This chronic inflammatory disorder of unknown etiology principally affects the axial skeleton. Alterations occur in synovial and cartilaginous articulations and in sites of tendon and ligament attachment to bone. Over 90 % of caucasian patients with ankylosing spondylitis are HLA-B27 positive.
Crystalline arthritis
Gout
This is the prototypic crystalline arthropathy, characterized by the deposition of monosodium urate crystals in the skin, subcutaneous tissues, and joints. This is most meaningfully classified as idiopathic gout, encompassing the vast majority of individuals, or gout associated with known disorders or enzymatic defects.
Calcium pyrophosphate crystal deposition disease
Calcium pyrophosphate crystal deposition disease: a general term for a disorder characterized by the deposition of calcium pyrophosphate dihydrate (CPPD) crystals in or around joints.
Pseudogout: a term applied to one of the clinical patterns that may be associated with CPPD crystal deposition disease. This pattern, characterized by intermittent acute attacks of arthritis, simulates the findings of gout.
Chondrocalcinosis: a term reserved for pathologically or radiologically evident calcification of hyaline articular cartilage or fibrocartilage. In some cases, this calcification may not indicate deposits of CPPD crystals but rather accumulations of some other crystal.
Pyrophosphate arthropathy: a term used to describe a peculiar pattern of structural joint damage occurring in CPPD crystal deposition disease simulating, in many ways, degenerative joint disease but characterized by distinctive features.
Hydroxyapatite deposition disease
This is a disorder characterized by recurrent painful periarticular calcium hydroxyapatite deposits in tendons and soft tissues.
Psoriatic arthritis
This is a relatively uncommon arthropathy which occurs in about 2 to 6 % of patients with psoriasis. Approximately 25 to 60 % of patients with psoriatic arthritis are HLA-B27 positive.
Reiter’s syndrome
Reiter’s syndrome is a relatively uncommon arthropathy of uncertain etiology with the classic triad of urethritis, arthritis, and conjunctivitis. Of all of the rheumatic diseases, Reiter’s syndrome is most suspect for an infectious etiology. It appears likely that the disease can be transmitted in association with either epidemic dysentery or sexual intercourse. The syndrome frequently follows an infection of the bowel or lower genitourinary tract, and it seems likely that these sites are the portals of entry for the causative agent. It has been suggested that the abnormalities of the vertebral column may be related to organisms extending directly to the sacroiliac joints and spine via the prostatic venous plexus or via the venous plexus of Batson. Implicated organisms include pleuropneumonia-like organisms (PPLO), the Bedsonia group of organisms, and viruses, although to date, no single agent has been definitely incriminated in this disease. Approximately 75 to 96 % of patients with Reiter’s syndrome are HLA-B27 positive.
Enteropathic arthropathy
This arthropathy occurs in about 1 – 26 % of patients with ulcerative colitis or Crohn’s disease. The relationship between inflammatory intestinal diseases and arthritis is not fully understood. Infectious, immunologic, and genetic etiologies have been advanced. Approximately 90 % of patients with ulcerative colitis or Crohn’s disease who develop spondylitis or sacroiliitis are HLA-B27 positive.
2. Radiographic Hallmarks
Osteophytes
In a diarthrodial joint, this is the sine qua non of osteoarthritis. Osteophytes can be seen in both primary and secondary osteoarthritis. They can also be seen at various entheses, often due to altered or increased stress at the entheses (traction osteophytes). The traction osteophytes of degenerative annular disease begin several millimeters from the edge of the vertebral body, and tend to be initially oriented horizontally at their attachment to the vertebral bodies. They then often curve slightly and may even form a complete bony bridge across the disc space.

bridging osteophytes in the spine of a patient with degenerative disk disease
Syndesmophytes
Syndesmophytes are generally seen only in the seronegative spondyloarthropathies. These are due to inflammation and ossification of the outer fibers of the annulus fibrosus, known as the Sharpey’s fibers. This is classically seen in ankylosing spondylitis. In the other seronegative spondyloarthropathies, one usually sees paravertebral ossification which forms in the paravertebral connective tissue at some distance from the spine. In practice, it may be very difficult to distinguish osteophytes from syndesmophytes or paravertebral ossification.

syndesmophytes (arrows) in the spine of a patient with ankylosing spondylitis
Disc space narrowing
This almost always means degenerative nuclear disease or infection. These can often be distinguished by looking at the adjacent endplates. In degenerative disc disease, the endplates are often dense, sclerotic, and associated with osteophytosis. In infection, the subchondral line of the endplate often becomes ill-defined and discontinuous.
Bony proliferation
This is a striking feature of the seronegative spondyloarthropathies, particularly psoriatic arthritis. This bony proliferation occurs about erosions, and probably relates to an exaggerated healing response of the injured bone. This proliferation may take the form of irregular excrescences, subperiosteal deposition of bone, and intra-articular osseous fusion.
Erosions
In general, the presence of erosions bespeaks some type of inflammatory disease, whether the erosions are due to synovial hypertrophy, crystalline deposits, or infection.
Crystal deposition
In general, this is indicative of one of the crystalline arthropathies — either CPPD or hydroxyapatite.
Sclerosis
Not an especially specific finding in spinal arthropathy.
Ankylosis
This may occur as a result of many degenerative and inflammatory processes in their later stages.
Subluxation
Stability of the spine is maintained by the spinal ligaments, articular capsules, and discs. Any arthropathy which causes degeneration or destruction of these structures may lead to instability of the spine and subluxation in several locations.
3. Pattern Approach
Osteoarthritis
Osteoarthritis of the spine looks much like osteoarthritis elsewhere in the body. Any of the spinal synovial joints can be affected, including the facet and uncovertebral joints, the costovertebral joints, and the SI joints. Findings include osteophytosis, joint space narrowing, subchondral sclerosis, and subchondral cyst formation. Besides causing local joint pain, facet osteoarthritis may cause nerve root impingement or compression if the osteophytes are large enough to extend into the lateral recess of the spinal canal, as shown below.

marked osteophytosis is seen in the spine of a patient with osteoarthritis of the lumbar facet joints — this osteophytosis is extending into the lateral recesses bilaterally and causing nerve root compression
Degenerative disc disease
Degeneration of either the nucleus pulposus, the annulus fibrosus, or both may be present. While these processes can often be distinguished from each other, overlap in findings will be seen in many patients who have both processes occurring in the same disc.
The key distinguishing characteristic between these two processes is disc space narrowing. If present, this is strongly suggestive of degenerative nuclear disease. This is often accompanied by endplate sclerosis and mild to moderate osteophytosis.
intervertebral disc space narrowing, intradiscal gas, and osteophytosis are noted in this patient with predominantly degenerative nuclear disease
On the other hand, degenerative annular disease is often not associated with significant disc space narrowing, and the marginal osteophytes seen with this entity are often much larger than those seen with degenerative nuclear disease.
extensive osteophytosis is noted in the thoracic spine in this patient with predominantly degenerative annular disease
DISH
With DISH, the flowing ossification seen is usually along the anterior longitudinal ligament. Although there has been recent speculation that DISH may be a disorder of vitamin A metabolism, DISH remains an idiopathic disorder. As such, it lacks not only a known specific cause but also a known specific disease marker (such as monosodium urate crystals in gout). Therefore, DISH is necessarily a diagnosis by exclusion. Since DISH is diagnosed on a morphologic basis alone, there will be of necessity some overlap between certain cases of DISH and other disorders with similar radiographic features, such as ankylosing spondylitis, and degenerative disc disease. To help minimize this overlap, certain arbitrary morphologic criteria have been proposed.
| Similar Disorders | Finding That Distinguishes Them From DISH |
| Ankylosing spondylitis | SI and facet joints must be normal |
| Degenerative nuclear disease | Disc spaces must be of normal height |
| Degenerative annular disease | Ossification must be seen along four contiguous vertebral bodies |
Since we often don’t have any specific therapy for DISH, is there any reason to try to distinguish it from all of these other disorders? I feel that there is. If for no other reason, knowing the name of a disease allows one to be much more precise in giving a prognosis to a patient. Knowledge of the presence of DISH may alter therapy for other disorders. For example, DISH patients are prone to heterotopic bone formation in surgical sites. Because of this, some orthopedic surgeons will prophylactically treat DISH patients with radiation or drug therapy prior to performing a total joint arthroplasty, in an attempt to prevent or diminish the development of heterotopic bone formation after surgery.



flowing ossification is noted along the anterior margin of the thoracic and lumbar spine in these patients with DISH — note that the disk spaces are preserved and that at least four contiguous bodies are involved
Ankylosing spondylitis
Ankylosing spondylitis affects synovial and cartilaginous joints as well as sites of tendon and ligament attachment to bone (entheses). An overwhelming predilection exists for involvement of the axial skeleton, especially the sacroiliac, apophyseal, discovertebral, and costovertebral articulations. Classically, changes are initially noted in the sacroiliac joints and next appear at the thoracolumbar and lumbosacral junctions. With disease chronicity, the remainder of the vertebrae may become involved. However, this characteristic pattern of spinal ascent is by no means invariable; it may occur slowly or rapidly, and is less frequent in spondylitis accompanying psoriasis and Reiter’s disease.
Sacroiliitis is the hallmark of ankylosing spondylitis. It occurs early in the course of the disease. Although an asymmetric or unilateral distribution can be evident on initial radiographic examination, roentgenographic changes at later stages of the disease are almost invariably bilateral and symmetric in distribution. This symmetric pattern is an important diagnostic clue in this disease and may permit it differentiation from other disorders that affect the sacroiliac articulation, such as RA, psoriasis, Reiter’s syndrome, and infection. Changes in the SI joint occur in both the synovial and ligamentous (superior) portions, and predominate on the iliac side, for reasons that are obscure.

bilateral erosions and sclerosis are noted in the SI joints of this patient with ankylosing spondylitis
The classic histologic descriptions of synovial joint alterations in ankylosing spondylitis stress that the synovitis is similar or identical to that in rheumatoid arthritis. Indeed, ankylosing spondylitis was once called rheumatoid spondylitis, under the impression that ankylosing spondylitis was just a variant of rheumatoid arthritis. Further research into this entity revealed enough clinical and immunological differences between the two entities to warrant calling it a disease of its own. In general, the inflammatory process in ankylosing spondylitis is more discrete and of lower intensity that in rheumatoid arthritis.

erosions are noted in the lumbar facet joints of this patient with ankylosing spondylitis
The characteristic radiographic features of ankylosing spondylitis include erosions, sclerosis, syndesmophytosis, and ankylosis.
Rheumatoid arthritis
As mentioned above, the histological changes noted classically in rheumatoid arthritis are similar or identical to those of ankylosing spondylitis. However, the general pattern of distribution of these changes are usually quite distinct from that of ankylosing spondylitis. For example, rheumatoid arthritis predominantly involves the cervical spine, with apophyseal joint erosion and malalignment, intervertebral disc space narrowing with endplate sclerosis and without osteophytes, and with multiple subluxations, especially at the atlanto-axial junction. Abnormalities of the thoracolumbar spine and sacroiliac joints are infrequent and less prominent than those of ankylosing spondylitis.

Other helpful differential findings are the absence of osteoporosis and the presence of bony proliferation and intraarticular bony ankylosis in the seronegative spondyloarthropathies.
CPPD crystal deposition disease
The spine is frequently involved in CPPD crystal deposition disease.
Intervertebral discal calcifications are frequent in the outer annular fibers, and may mimic early syndesmophytes of ankylosing spondylitis, because of their vertical orientation and slender appearance. These annular calcifications may be associated with back pain. Disc space narrowing is common in CPPD crystal deposition disease, and may be extensive, widespread, and associated with considerable vertebral sclerosis. However, the nucleus pulposus is not commonly calcified. Calcification of ligamentum flavum may also be noted. Occasionally, destructive abnormalities of cervical spine are present. Chondrocalcinosis is only infrequently seen in the sacroiliac joints, but is very common in the fibrocartilaginous joint of the pubic symphysis.
Gout
Spinal manifestations of gout are extremely uncommon, and documented urate deposition in the spine is exceedingly rare. When seen, spinal gout may manifest as erosions of the synovial joints or endplates, and disc space narrowing may be present.
The incidence of gout in the sacroiliac joint has been reported at 7 – 17 %, although many of the changes ascribed to gout in the earlier literature were probably mimicked in these reports by the changes of osteoarthritis. Sacroiliac joint involvement is seen more frequently with early onset disease, and large cystic areas of erosion in ilium and sacrum are the most specific findings of gout in these joints.
Hydroxyapatite crystal deposition disease
Hydroxyapatite crystal deposition disease is most commonly seen about the shoulder. However, it may also occur within the longus colli muscle, which is the principal flexor of the cervical spine. Tendinitis in this region may result in acute neck and occipital pain, rigidity, and dysphagia. Calcifications tend to occur particularly in the superolateral group of the longus colli. The typical radiographic findings of this disorder consist of prevertebral soft tissue swelling in upper cervical region, as well as amorphous calcification, usually anterior to C-2, and just below the anterior arch of C-1. Resorption of this calcification and soft tissue swelling is common, and it may disappear completely in 1 to 2 weeks.
Psoriatic arthritis
About 30 to 50 % of patients with psoriatic arthritis develop sacroiliac joint changes radiographically. Bilateral sacroiliac joint abnormalities are much more frequent than unilateral changes, and although asymmetric findings may be apparent, symmetric abnormalities predominate. Radiographic sacroiliac joint changes include erosions and sclerosis, predominantly on the iliac side, and widening of the articular space. Although significant joint space diminution and bony ankylosis can occur, the incidence of these findings, particularly ankylosis, is less than that of classic ankylosing spondylitis or the spondylitis associated with inflammatory bowel disease. Sacroiliitis may appear without spondylitis, just as spondylitis may appear without sacroiliitis.
As in Reiter’s syndrome, paravertebral ossification about the lower thoracic and upper lumbar segments can occur in psoriatic arthritis, and it may represent an early manifestation of the disease. Such ossification appears as a thick and fluffy or thin and curvilinear radiodense region on one side of the spine, paralleling the lateral surface of the vertebral bodies and the intervertebral discs. Occasionally, slender, centrally located, and symmetric spinal outgrowths in psoriasis are identical in appearance to the syndesmophytes of ankylosing spondylitis. However, the greater size, the unilateral or asymmetric distribution, and the location farther away from the vertebral column are features that distinguish paravertebral ossification from the typical syndesmophytosis of ankylosing spondylitis or the spondylitis of inflammatory bowel disease.
In addition to the pattern and distribution of bony outgrowths, there are other features of psoriatic spondylitis that differ from those in classic ankylosing spondylitis. Osteitis and squaring of the anterior surfaces of the vertebral bodies are relatively infrequent in psoriasis. Although apophyseal joint space narrowing, sclerosis and bony ankylosis may be seen, the prevalence of these findings is much less than that in ankylosing spondylitis.
Cervical spine abnormalities may be striking in psoriatic arthritis, including apophyseal joint space narrowing and sclerosis, osseous irregularity at the discovertebral joint, and extensive proliferation along the anterior surface of the spine. Atlanto-axial subluxation can also be evident (in one series up to 45 % of patients with psoriatic spondylitis).
Reiter’s syndrome
Reiter’s syndrome is associated with an asymmetric arthritis of the lower extremity, sacroiliitis, and, less commonly, spondylitis. Although its general features resemble those of ankylosing spondylitis and psoriatic arthritis, Reiter’s syndrome possess a sufficiently characteristic articular distribution to allow accurate diagnosis.
Ankylosing spondylitis has a similar axial skeletal distribution (although cervical changes are more frequent in ankylosing spondylitis), but significant peripheral articular changes are more frequent.
Psoriatic arthritis may lead to considerable alterations in the articulations of both the appendicular and the axial skeleton. However, in psoriasis, widespread involvement of the upper extremity may be apparent, and distal interphalangeal joint abnormalities in both upper and lower extremities are common. The sacroiliac and spinal changes of Reiter’s syndrome are virtually identical to those of psoriasis, although the incidence and severity of these abnormalities and the tendency to involve the cervical spine are greater in psoriasis.

sclerosis and ill-definition of both SI joints is noted in this patient with Reiter’s syndrome

Enteropathic arthropathy
The spondylitis and sacroiliitis of inflammatory bowel disease are identical to those of classic ankylosing spondylitis. The history of inflammatory bowel disease can sometimes help to distinguish these entities, although spondylitis in ulcerative colitis is poorly correlated with activity of the bowel disease. In ulcerative colitis, spinal abnormalities may become manifest prior to, at the same time as, or following the onset of intestinal changes. In fact, spondylitis most commonly precedes the onset of colitis and may progress relentlessly without relation to exacerbation, remission, or treatment of the bowel disease. In Crohn’s disease, the joint abnormalities tend to occur simultaneously with the bowel disease.
Peripheral joint abnormalities tend to occur much more frequently with enteropathic arthropathy than with ankylosing spondylitis. When they do occur, they are usually self limited, and rarely cause lasting deformity of the joint. However, in ankylosing spondylitis, the peripheral joint findings typically include joint space narrowing, osseous erosions, cysts, and bony proliferation, which may help in distinguishing these entities.
4. Demographics
All of the entities described in this section on axial arthropathies can occur in the young or the old, and in men or women. However, just as in the appendicular arthropathies, there are certain trends in the distribution of these disorders that may sometimes be helpful in refining one’s differential diagnosis. The following tables show some of these trends. As with the appendicular arthropathies, other demographic features such as home location, occupation, and ethnic subtype may occasionally be of help.
| Age | ||
| Age Group | Age of Onset | Disorder |
| Young (< 20 years) | < 20 years | Juvenile chronic arthritis Septic arthritis |
| Middle (> 20 years) | onset 15 – 35 years | Ankylosing spondylitis Reiter’s |
| Young adults | Enteropathic arthropathies | |
| 25 – 55 years | Rheumatoid arthritis Psoriatic arthritis |
|
| Older patients (> 55 years) | > 55 years | Osteoarthritis DISH CPPD |
| Arthropathies with Male Predominance | |
| Disorder | male:female ratio |
| Ankylosing spondylitis | 4:1 to 10:1 |
| Psoriatic | 2:1 to 3:1, but controversial |
| Reiter’s | 5:1 to 50:1 |
| Gout | 20:1 |
| DISH | 3:2 |
| CPPD | 1:1 |
| Primary osteoarthritis (< 45 years) |
|
| Enteropathic arthropathy | |
| Ulcerative colitis | 4:1 |
| Crohn’s disease | 1:1 |
Arthropathies with Female Predominance
| Disorder | female:male ratio |
| Rheumatoid Arthritis | 2:1 to 3:1 |
| Primary osteoarthritis (> 45 years) |
|
| CPPD | 1:1 |
5. The law of parsimony
As in the appendicular arthropathies, a patient may have more than one arthropathy going on in a given joint. Again, this is most commonly due to secondary osteoarthritis due to some other arthropathy, although other unusual combinations of arthropathies may be seen. This principle can sometimes help to clarify what otherwise might be a confusing radiographic picture.