Teaching Files
Archived Case 50
Contributed by: Katherine E. Dee, MD -
Screening: See question below.
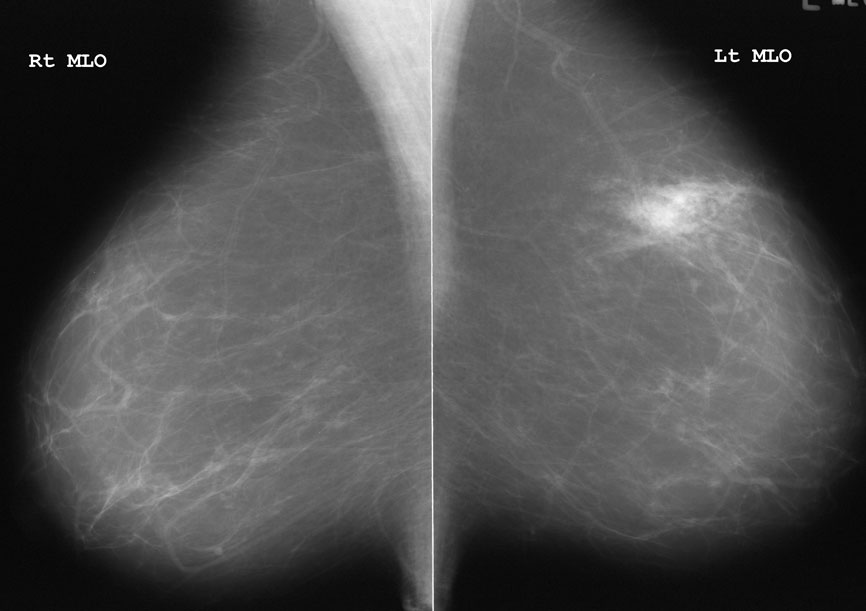
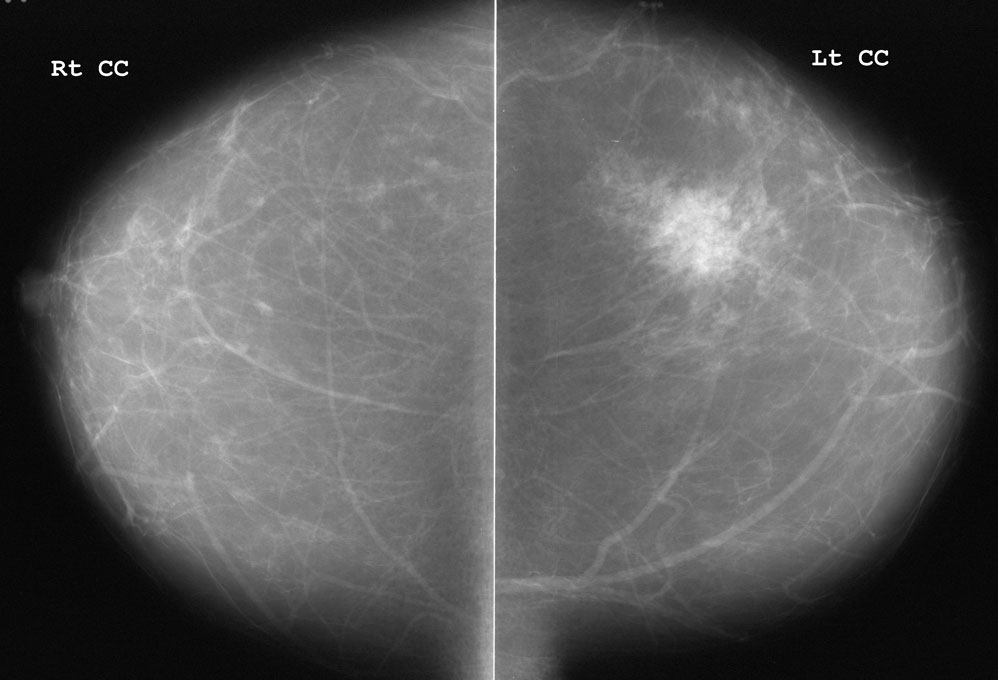
What is your assessment?
BI-RADS 0 - IncompleteBI-RADS 1 - Normal
BI-RADS 2 - Benign
BI-RADS 3 - Probably Benign
BI-RADS 4 - Suspicious
BI-RADS 5 - Highly Suggestive of Malignancy