Teaching Files
Archived Case 30
Contributed by: Katherine E. Dee, MD -
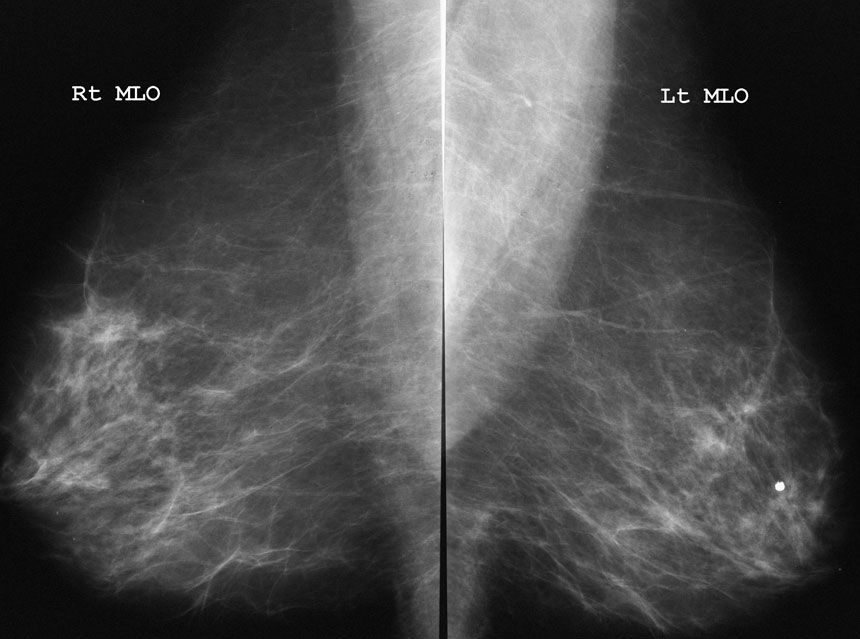
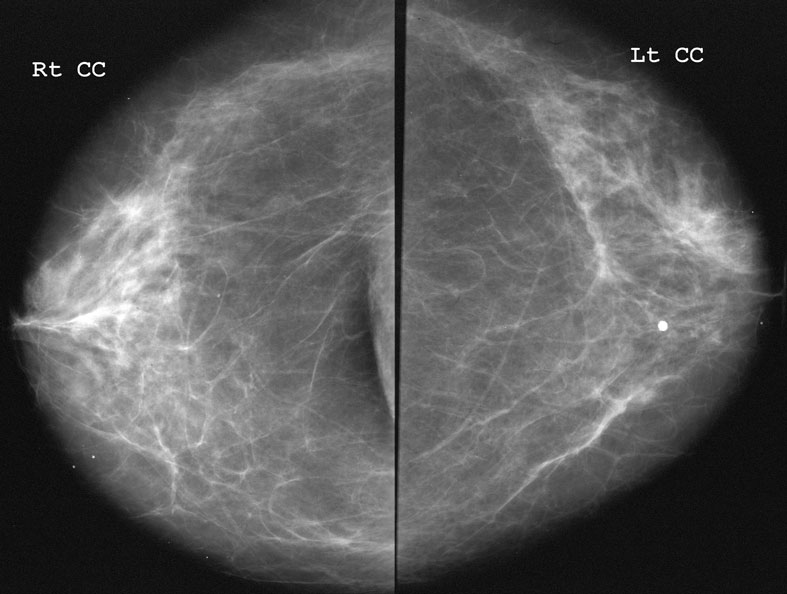
Screening Mammogram
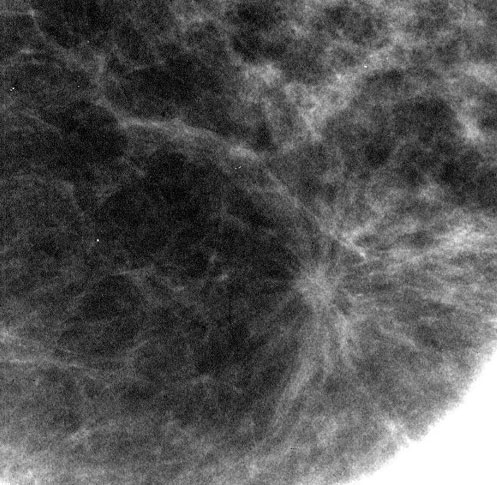
Spot compression magnification view:
What is the most likely pathologic diagnosis?
FibrosisDCIS
Mucinous Carcinoma
Radial Scar
This finding is focal architectural distortion without a central density or mass. One could argue that there may be a tiny 2mm spiculated mass on the CC spot mag, but this could not be shown on MLO or Lat views (take another look at the MLO view).
Though this area could represent fibrosis, this would be unlikely since fibrosis rarely causes spiculations seen in this case. This would be an extremely unusual presentation for DCIS, which rarely causes architectural distortion, especially in such a focal manner. Mucinous carcinomas generally present as a mass.
Now if tubular carcinoma had been an option, that would also be possible. Tubular carcinomas are low-grade and tend to present as small spiculated masses.
What is your assessment?
BI-RADS 2 - Benign - Recommend 12 month follow-upBI-RADS 3 - Probably Benign - Recommend 6 month follow-up
BI-RADS 4 - Suspicious - Recommend core needle biopsy
BI-RADS 4 - Suspicious - Recommend wire localization and surgical excision
BI-RADS 5 - Highly Suggestive of Malignancy - Recommend wire localization and surgical excision
Answers D and E can also be correct. A core biopsy can provide a diagnosis to assist with treatment planning if cancer is present. Studies show that patients who have needle biopsies will undergo fewer expensive surgeries for definitive therapy. Some institutions will recommend excision of this lesion immediately because regardless of the core needle biopsy result the lesion needs to be removed. Radial scars have an association with tubular carcinomas about 20% of the time. They are also notoriously difficult to diagnose from a needle biopsy (just ask your local pathologist!) This did turn out to be a radial scar, in case you’re keeping track.
Our surgeons at UW prefer that we attempt a core biopsy prior to excision (a cancer diagnosis prior to surgery will change surgical management– the surgeon will attempt to get clean margins and will perform a sentinel node biopsy).
As I have mentioned before (see Case 2) some mammographers prefer to call these lesions BI-RADS 5, to be sure to convey the need for excision. Since I know I’d be eating my hat over these most of the time, I prefer to call it BI-RADS 4. As long as you communicate your recommendations clearly, this should not be a problem.