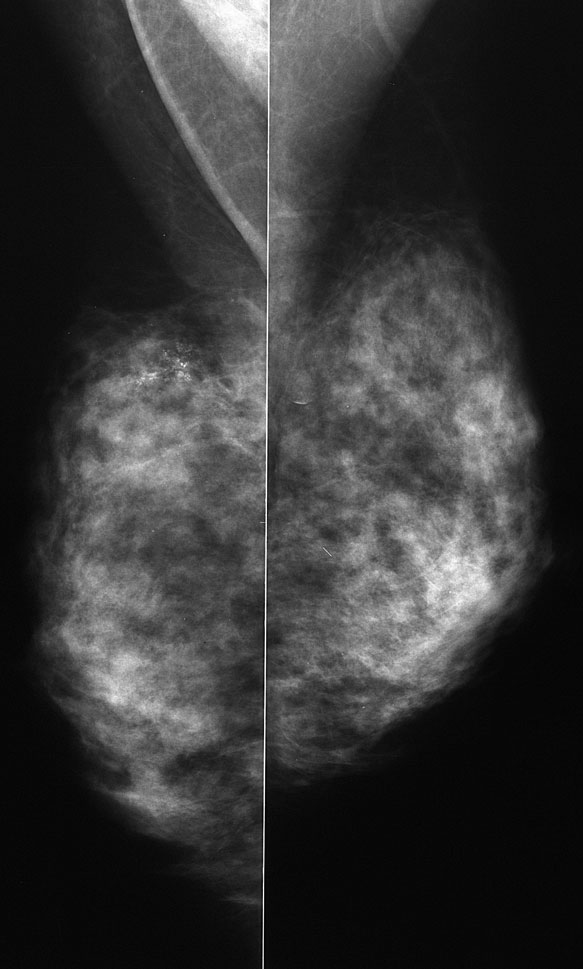
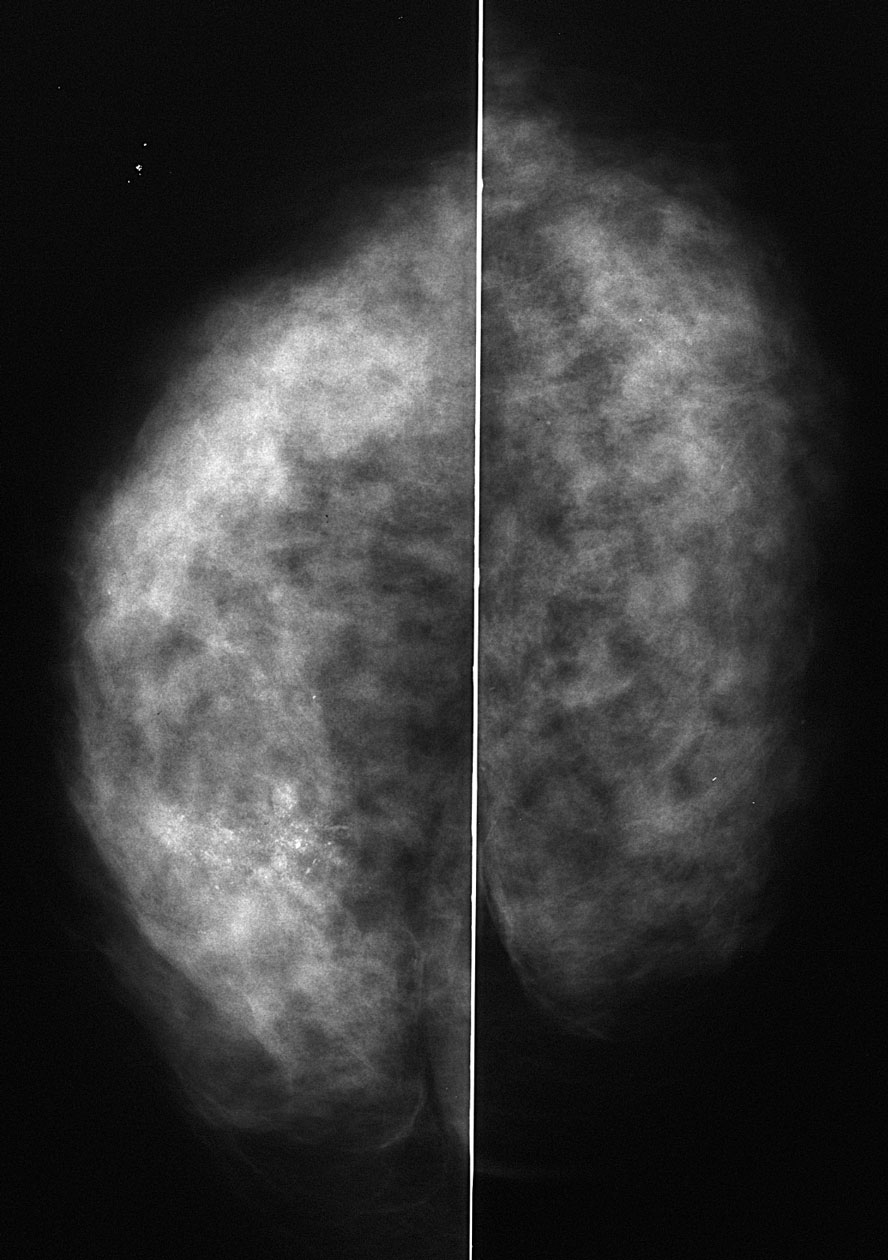
A cluster of calcifications are present in the upper inner right breast. This case was classified as BI-RADS 0, and the patient returned for spot compression magnification views.
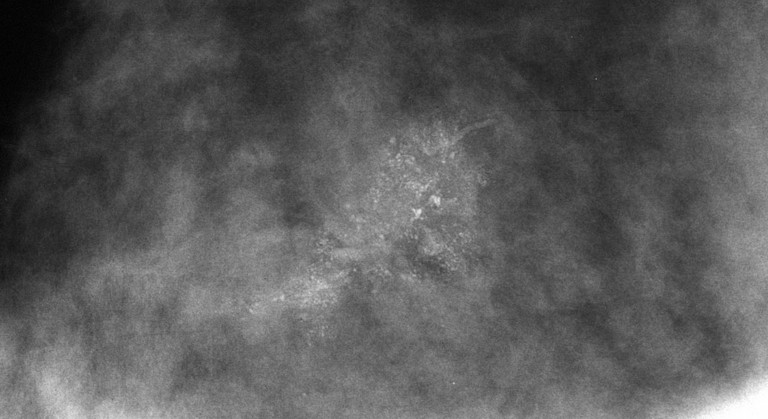
These calcifications are clustered and pleomorphic. If you said BI-RADS 5, that is acceptable. As has been mentioned in earlier cases, many mammographers use BI-RADS 5 only when they are sure that the finding is cancer. Therefore, I would not use BI-RADS 5 in this particular case.
The patient was scheduled for a stereotactic biopsy. What approach would you use?
Superior - Craniocaudal Lateral - ML Medial - ML Inferior - Caudocranial
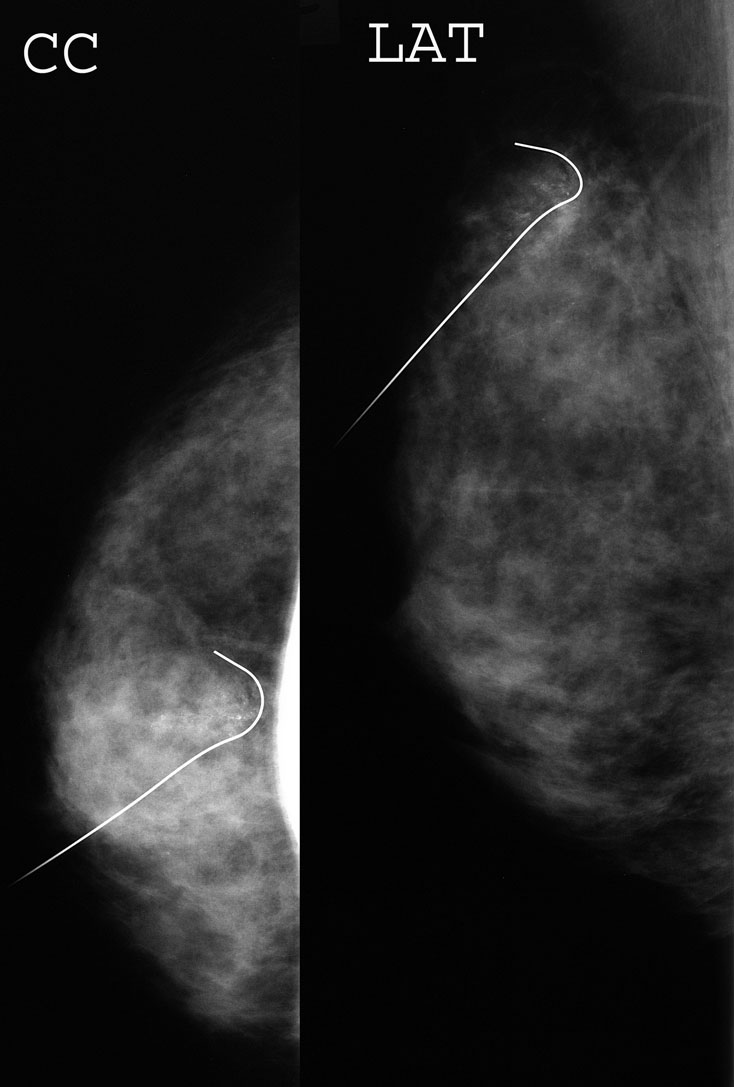
The stereotactic biopsy was performed using a superior approach with the CC view as a guide
The calcifications were closest to the superior skin. This minimizes the distance traversed by the needle from the skin to the target.
Other considerations when deciding the approach:
1. Is the finding seen much more easily on one of the views? Then the approach in that view may be necessary, even if the distance is farther.
2. Do anatomic conditions make only one approach possible?
3. Is a vessel overlying the finding in one of the views?
4. Does the patient have a strong preference for where the small potential scar might be located?
The biopsy yielded DCIS. What is your recommendation now?
6 month mammograms to closely screen for an invasive tumor wire localization and surgical excision breast MRI to evaluate extent of disease and consultation with surgical oncology and medical oncology mastectomy
Breast MRI and consultation with surgical oncology and medical oncology are recommended.
The standard of care in the United States is to treat DCIS as a cancer. MRI demonstrates the extent of disease better than mammography or ultrasound. Surgery can be either lumpectomy to obtain clean margins followed by radiation therapy OR mastectomy without radiation therapy
Is a specimen radiograph necessary?
Yes No
Yes
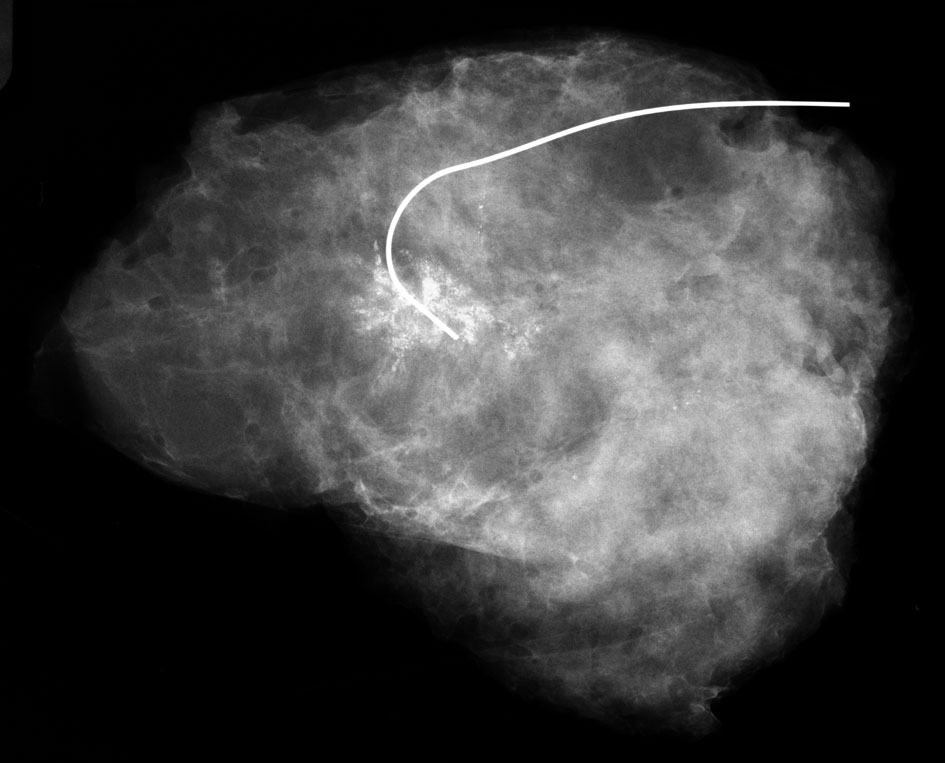
A specimen radiograph is obtained before closing to confirm that the target has been removed. In addition, if the specimen radiograph shows a close margin, the surgeon will be able to excise that margin at the time of lumpectomy. This decreases the chances of re-operation for positive margins. Many sites perform 2 orthogonal views of the specimen to more completely assess margins.
In this case, the calcifications have been completely removed, and are well within the radiographic margins