About Us
58 year-old who became acutely unresponsive while talking on the phone
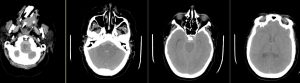
CT noncontrast
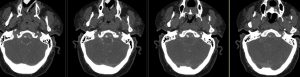
CTA axial source images
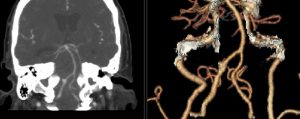
CTA coronal and 3D recons
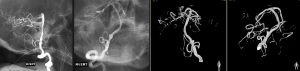
Right vertebral artery injection lateral, AP, and 3D recons
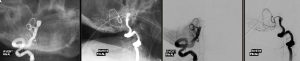
Right Vertebral artery injection AP and lateral views s/p coiling
Findings:
CT: diffuse subarachnoid hemorrhage CTA and angiogram: Right vertebral artery focal enlargement just distal to the PICA origin involving the anterior spinal artery origin
DDX:
Fusiform aneurysm, dissecting aneurysm, FMD
Diagnosis:
Right vertebral artery dissecting aneurysm just distal to the PICA origin involving the anterior spinal artery
Discussion:
A vertebral artery dissection usually begins with an expanding hematoma in the vessel wall. This intramural hematoma can arise spontaneously or secondary to minor trauma. It also can be introduced through an intimal flap that develops at the level of the inner lumen of the vessel. Subadventitial dissections tend to cause pseudoaneurysmal dilation of the vertebral artery, which may compress adjacent neurologic structures. These subadventitial dissections are prone to rupture through the adventitia, resulting in subarachnoid hemorrhage. In an autopsy series of more than 100 patients with subarachnoid hemorrhage, 5% of the hemorrhages were from vertebral dissection. Due to their natural history to rebleed, rapid treatment, often with coil embolization is favored. In this case, a risk factor was the presence of the anterior spinal artery origin within the dissection. Fortunately, after coiling there was retrograde filling of the anterior spinal artery via muscular perforators from the proximal right vertebral artery.
Submitted by Dinesh Rao, MD, UW Neuroradiology Fellow